Oral use.
Individual dose titration against efficacy and tolerability is recommended. REQUIP PD 24 HOUR prolonged-release tablets should be taken once a day and at a similar time each day. The tablets must be swallowed whole and must not be chewed, crushed or divided. The tablets may be taken with or without food (see Pharmacology: Pharmacokinetics under Actions).
Adults: Initial titration: The starting dose of REQUIP PD 24 HOUR prolonged-release tablets is 2 mg once daily for the first week; this should be increased to 4 mg once daily from the second week of treatment. A therapeutic response may be seen at a dose of 4 mg once daily of REQUIP PD 24 HOUR prolonged-release tablets.
Patients who initiate treatment with a dose of 2 mg/day of ropinirole prolonged-release tablets and who experience side effects that they cannot tolerate, may benefit from switching to treatment with REQUIP IR (immediate release) tablets at a lower daily dose, divided into three equal doses.
Therapeutic regimen: Patients should be maintained on the lowest dose of REQUIP PD 24 HOUR prolonged-release tablets that achieve symptomatic control.
If sufficient symptomatic control is not achieved or maintained at a dose of 4 mg once daily of REQUIP PD 24 HOUR prolonged-release tablets, the daily dose may be increased by 2 mg at weekly or longer intervals up to a dose of 8 mg once daily of REQUIP PD 24 HOUR prolonged-release tablets.
If sufficient symptomatic control is still not achieved or maintained at a dose of 8 mg once daily of REQUIP PD 24 HOUR prolonged-release tablets, the daily dose may be increased by 2 mg to 4 mg at two weekly or longer intervals. The maximum daily dose of REQUIP PD 24 HOUR prolonged-release tablets is 24 mg.
It is recommended that patients are prescribed the minimum number of REQUIP PD 24 HOUR prolonged-release tablets that are necessary to achieve the required dose by utilising the highest available strengths of REQUIP PD 24 HOUR prolonged-release tablets.
When REQUIP PD 24 HOUR prolonged-release tablets are administered as adjunct therapy to levodopa, it may be possible to gradually reduce the levodopa dose, depending on the clinical response. In clinical trials, the levodopa dose was reduced gradually by approximately 30% in patients receiving REQUIP PD 24 HOUR prolonged-release tablets concurrently. In patients with advanced Parkinson's disease receiving REQUIP PD 24 HOUR prolonged-release tablets in combination with L-dopa, dyskinesias can occur during the initial titration of REQUIP PD 24 HOUR prolonged-release tablets. In clinical trials it was shown that a reduction of the L-dopa dose may ameliorate dyskinesia (see Adverse Reactions).
When switching treatment from another dopamine agonist to ropinirole, the marketing authorisation holder's guidance on discontinuation should be followed before initiating ropinirole.
As with other dopamine agonists, it is necessary to discontinue ropinirole treatment gradually by reducing the daily dose over the period of one week (see Precautions).
Switching from REQUIP immediate release (IR) tablets to REQUIP PD 24 HOUR prolonged-release tablets: Patients may be switched overnight from REQUIP IR tablets to REQUIP PD 24 HOUR prolonged-release tablets.
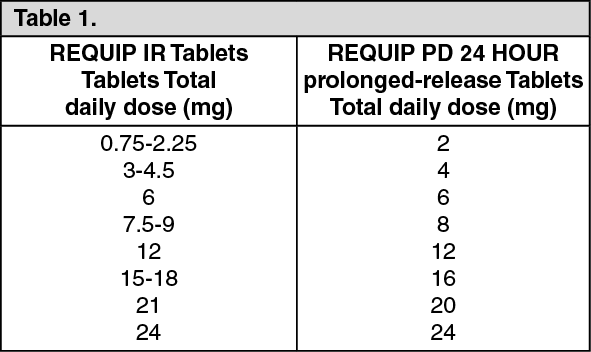
The dose of REQUIP PD 24 HOUR prolonged-release tablets should be based on the total daily dose of REQUIP IR tablets that the patient was receiving. The recommended dose for switching from REQUIP IR tablets to REQUIP PD 24 HOUR prolonged-release tablets are provided in the following table. If patients are taking a different total daily dose of REQUIP IR tablets to those typically prescribed doses as shown in the table, they should be switched to the nearest available dose of REQUIP PD 24 HOUR prolonged-release tablets as stated in the table: (see Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
After switching to REQUIP PD 24 HOUR prolonged-release tablets, the dose may be adjusted depending on the therapeutic response (see "Initial titration" and "Therapeutic regimen" as previously mentioned).
Dose interruption or discontinuation: If treatment is interrupted for one day or more, re-initiation by dose titration on REQUIP IR tablets should be considered.
If it is necessary to discontinue ropinirole treatment, this should be done gradually by reducing the daily dose over the period of one week.
Renal impairment: In parkinsonian patients with mild to moderate renal impairment (creatinine clearance between 30 and 50 ml/min) no change in the clearance of ropinirole was observed, indicating that no dosage adjustment is necessary in this population.
A study into the use of ropinirole in patients with end stage renal disease (patients on haemodialysis) has shown that a dose adjustment in these patients is required as follows: The recommended initial dose of REQUIP PD prolonged-release tablets is 2 mg once daily. Further dose escalations should be based on tolerability and efficacy. The recommended maximum dose is 18 mg/day in patients receiving regular dialysis. Supplemental doses after dialysis are not required.
The use of ropinirole in patients with severe renal impairment (creatinine clearance less than 30 ml/min) without regular haemodialysis has not been studied.
Hepatic impairment: The use of ropinirole in patients with hepatic impairment has not been studied. Administration of ropinirole to such patients is not recommended.
Elderly: The clearance of ropinirole is decreased by approximately 15% in patients aged 65 years or above. Although a dose adjustment is not required, ropinirole dose should be individually titrated, with careful monitoring of tolerability, to the optimal clinical response. In patients aged 75 years and above, slower titration during treatment initiation may be considered.
Children and adolescents: REQUIP PD 24 HOUR prolonged-release tablets are not recommended for use in children below 18 years of age due to a lack of data on safety and efficacy.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image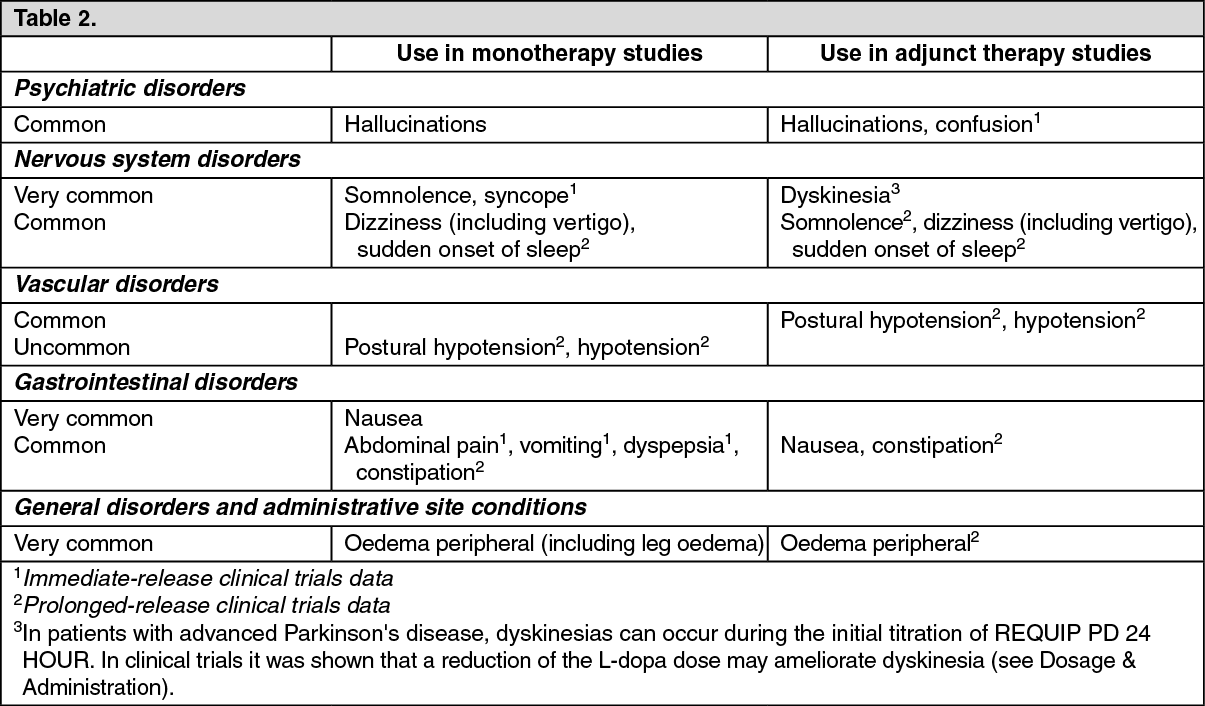 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
